Achalasia is a rare but serious disorder of the esophagus that affects the ability of the esophagus to move food toward the stomach. It is a progressive condition that typically develops gradually over time, causing increasing difficulty swallowing, regurgitation, chest discomfort, and weight loss. Understanding the stages of achalasia — from early presentation to end-stage disease — is crucial for timely diagnosis, appropriate management, and preventing severe complications.
We will explore what differentiates Stage 1 achalasia from Stage 4 achalasia, how the disease progresses through defined stages, the clinical implications of this progression, how the stages are diagnosed, and contemporary treatment strategies tailored to each stage.
Introduction: What Is Achalasia?
Achalasia is a chronic motility disorder of the esophagus characterized primarily by:
- Loss of normal esophageal peristalsis (the rhythmic muscle contractions that push food downward).
- Failure of the lower esophageal sphincter (LES) — the muscle that separates the esophagus from the stomach — to relax properly.
This combination leads to difficulty swallowing (dysphagia), retention of food and liquid in the esophagus, and progressively worsening symptoms if left untreated.
Although achalasia is most reliably diagnosed with esophageal manometry (a measurement of muscle activity in the esophagus), imaging studies such as barium swallow X-rays and endoscopy are also key tools for characterizing the anatomical changes that occur as the disease advances.
One way clinicians describe the evolution of achalasia is through staging — a framework that reflects the anatomical and functional severity of the disorder. While clinical subtypes based on manometry exist (Type I, II, and III), radiological staging systems based on esophageal morphology provide valuable insight into disease progression and guide appropriate treatment decisions.
Understanding the Staging System for Achalasia
The term “stages of achalasia” commonly refers to the radiological grading of how dilated and structurally altered the esophagus has become over time. The most widely referenced staging framework classifies achalasia into four stages based on the esophageal diameter and shape as seen on imaging such as a barium swallow study.
Stage 1: Early or Minimal Disease
- Esophageal diameter: ≤ 4 cm
- Shape: Straight or near-normal
- Motility: Mild or early dysfunction
- Symptoms: Minimal to mild
In Stage 1 achalasia, the esophagus may be only slightly dilated, and some degree of peristalsis (though impaired) may still be present. Importantly, the diameter of the esophagus remains ≤ 4 cm, and there is little to no structural deformity.
Clinically, patients in this stage may have complaints of occasional difficulty swallowing solid foods. The symptoms might be subtle and intermittent, and many individuals do not yet show severe functional impairment that significantly disrupts quality of life.
Despite being early, this stage is critical in terms of diagnosis because early treatment can prevent progression. Patients may undergo remedies such as lifestyle modifications, pharmacotherapy (e.g., calcium channel blockers or nitrates), or endoscopic balloon dilation, depending on symptom severity and clinician judgment.
Stage 2: Moderate Dilation
- Esophageal diameter: ~4–6 cm
- Shape: Still straight, but more distended
- Symptoms: Increasing dysphagia and regurgitation
In Stage 2 achalasia, the esophageal body becomes more prominently dilated — roughly between 4 and 6 cm in diameter. Although the esophagus still maintains a straight course, the increased enlargement reflects a more significant hindrance to food transit.
Symptoms at this stage become more noticeable and troublesome. Patients often describe constant difficulty swallowing both liquids and solids, with increased episodes of regurgitation of undigested food. Weight loss may also begin as patients unconsciously modify their eating habits to cope.
Treatment at this stage may involve more aggressive interventions, such as balloon dilation or surgical myotomy (cutting the LES muscle to reduce sphincter pressure), to improve esophageal emptying and reduce symptoms.
Stage 3: Advanced Disease
- Esophageal diameter: ≥ 6 cm
- Shape: Straight or mildly enlarged
- Symptoms: Severe dysphagia, high food retention
Stage 3 marks a shift toward more advanced disease. The esophagus is markedly dilated (typically ≥ 6 cm in diameter), though it may still be relatively straight in configuration. The significantly increased size reflects ongoing dysfunction of the LES and progressive loss of peristalsis, resulting in substantial retention of food and fluid.
Symptoms at this stage often include:
- Severe dysphagia to both liquids and solids
- Frequent regurgitation
- Significant weight loss
- Risk of aspiration (inhalation of food particles into the lungs)
Patients at Stage 3 often require more comprehensive treatment, which might include myotomy (surgical or endoscopic) to alleviate obstruction at the LES and augment esophageal emptying.
Stage 4: End-Stage Achalasia
- Esophageal diameter: ≥ 6 cm
- Shape: Sigmoid (twisted or tortuous)
- Symptoms: Severe and potentially life-limiting
Stage 4 achalasia — also referred to as end-stage achalasia — represents the most advanced form of the disease. Here, the esophagus not only exhibits significant dilation (often >6–8 cm), but also becomes sigmoid or tortuous in shape, bending within the chest due to progressive remodeling of the esophageal wall.
Functionally, the esophagus at this point behaves almost like a static reservoir rather than a muscular conduit, making food passage into the stomach extremely limited even with aggressive therapies designed to relax the LES. Late complications include:
- Persistent regurgitation and aspiration risk
- Severe malnutrition due to inability to eat sufficient calories
- Respiratory infections from aspiration
- Chronic esophagitis and inflammation
Many patients with Stage 4 achalasia are poor candidates for simple dilation or myotomy, as the structural deformities of the esophagus may prevent meaningful functional improvement with these approaches.
Instead, surgical removal of the esophagus (esophagectomy) with reconstruction is often considered the most effective treatment, albeit with significant surgical risk.
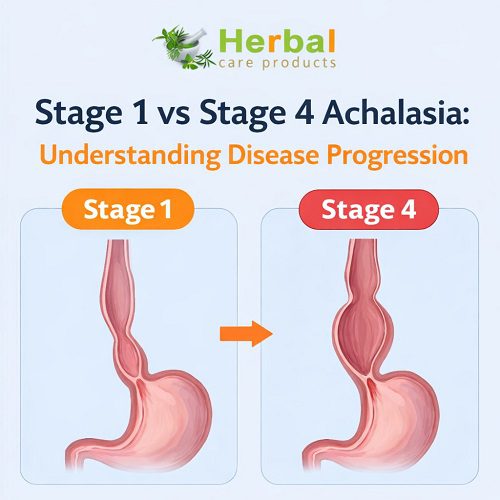
Stage 1 vs Stage 4: Key Differences
To understand the contrast between Stage 1 and Stage 4 achalasia, it helps to highlight their differences in terms of anatomy, symptoms, disease mechanisms, and therapeutic implications:
Esophageal Structure
- Stage 1: Minor dilation (≤ 4 cm), straight esophagus.
- Stage 4: Severe dilation (>6 cm) with sigmoid deformity.
Functional Impairment
- Stage 1: Partial impairment of LES relaxation with early peristaltic abnormalities.
- Stage 4: Near-complete loss of peristalsis and massive outflow obstruction despite spasm relief.
Symptoms
- Stage 1: Mild dysphagia, occasional regurgitation.
- Stage 4: Severe, constant dysphagia; food retention; high aspiration and malnutrition risk.
Treatment Options
- Stage 1: Conservative measures, dilation, targeted pharmacotherapy.
- Stage 4: Often surgical esophagectomy due to irreversible structural changes.
How Achalasia Progresses Through Stages
Achalasia does not develop overnight. It typically starts with subtle symptoms and slowly progresses as the nerve cells that control esophageal motility deteriorate. This neuronal damage — where the ganglion cells of the myenteric plexus are lost — leads to reduced peristalsis and impaired LES relaxation. Over time, the esophagus becomes increasingly atonic and dilated.
While the exact rate of progression varies widely among individuals, several factors can influence how quickly achalasia advances from Stage 1 toward Stage 4:
- Delayed Diagnosis or Inadequate Treatment: Patients who go years without effective treatment are far more likely to develop advanced disease.
- Failure of Therapy: Suboptimal response to interventions such as balloon dilation or myotomy can allow structural damage to continue.
- Recurrent Disease After Treatment: Even after initial symptom relief, achalasia can recur and worsen without surveillance.
- Secondary Causes: Infections (e.g., Chagas disease) and certain malignancies can accelerate dysfunction.
Because of its potential for progression, early diagnosis and intervention are key goals in clinical care.
Diagnosis: How Clinicians Determine Stages
Clinicians use a combination of tests to determine the disease stage and subtypes of achalasia:
1. Esophageal Manometry
This test remains the gold standard for diagnosing achalasia by measuring pressures in the esophagus. It helps define functional subtypes, but does not necessarily provide detailed structural staging. However, severe functional loss often correlates with advanced structural disease.
2. Barium Swallow Study
A barium swallow X-ray is central to defining the stages of achalasia based on esophageal diameter and shape: a straight narrow esophagus in early stages versus a markedly dilated, sigmoid shape in late stages.
3. Endoscopy
Endoscopy is crucial to rule out pseudoachalasia — obstruction caused by cancer or other growths — but may also visually confirm esophageal retention of food in advanced cases.
4. CT Scanning
CT imaging may be used when there is concern about complications or structural abnormalities, especially in advanced disease with significant dilation.
Treatment Strategies by Stage
Early Stage (Stage 1)
- Lifestyle and Diet: Eating slowly, chewing thoroughly, avoiding large meals.
- Medications: Smooth muscle relaxants in selected cases.
- Endoscopic Interventions: Pneumatic balloon dilation can be effective in reducing LES pressure.
- Myotomy: Endoscopic (POEM) or surgical myotomy may be considered if symptoms persist.
Moderate to Advanced Stages (Stages 2–3)
- Endoscopic Dilation: Often repeated to improve LES opening.
- POEM (Per-oral Endoscopic Myotomy): Increasingly popular and effective for moderate disease.
- Laparoscopic Heller Myotomy: Classic surgical approach for symptom relief.
End Stage (Stage 4)
- Esophagectomy: Often recommended because of irreversible dilation and tortuosity.
- Nutritional Support: Preoperative optimization due to malnutrition risks.
- Aspiration Prevention: Frequent monitoring due to high aspiration risk.
Conclusion: Why Early Recognition Matters
Understanding the stages of achalasia — particularly the meaningful differences between Stage 1 and Stage 4 — highlights the importance of early detection and intervention. Early in the disease course, when the esophagus is minimally dilated and symptoms are mild, interventions can be highly effective and may prevent irreversible structural damage.
In contrast, Stage 4 achalasia reflects end-stage disease with severe anatomical deformity and functional loss, often requiring major surgery and associated with significant morbidity.
If you or someone you know experiences progressive swallowing difficulties or persistent gastrointestinal symptoms, timely evaluation by a specialist — including manometry and imaging — can make a critical difference in outcomes.
You can visit our product page to explore more about this disease: “https://www.herbal-care-products.com/product/achalasia/”