Understanding the difference between achalasia vs GERD is critical for patients experiencing chronic esophageal symptoms. While both conditions affect the esophagus, they have distinct causes, symptoms, diagnostic pathways, and treatments. Misdiagnosis can lead to ineffective therapy and prolonged discomfort, which is why distinguishing these two conditions early is essential. This article explores the nuances of achalasia vs GERD in detail.
What is Achalasia?
Achalasia is a rare esophageal motility disorder that affects the lower esophageal sphincter (LES), preventing it from relaxing properly during swallowing. This dysfunction results in difficulty in moving food from the esophagus into the stomach.
Causes of Achalasia
The exact cause of achalasia is not fully understood, but research suggests:
- Nerve damage: Loss of nerve cells in the esophagus, particularly the myenteric plexus.
- Autoimmune factors: Some evidence points to the immune system attacking esophageal neurons.
- Infections: Rarely, viral infections may trigger nerve damage.
- Genetic predisposition: Although uncommon, certain genetic factors can increase susceptibility.
Symptoms of Achalasia
Achalasia typically presents gradually, and patients often confuse its symptoms with acid reflux. Common signs include:
- Difficulty swallowing (dysphagia): Both solids and liquids.
- Regurgitation: Undigested food or saliva coming back up without nausea.
- Chest pain: Often due to esophageal spasms.
- Weight loss: From prolonged difficulty eating.
- Nocturnal cough or aspiration: Food refluxing into the lungs during sleep.
Unlike GERD, heartburn is less prominent in achalasia, though some patients may experience mild discomfort.
Well, If you want to take best care of your digestive health or overcome the symptoms of achalasia. You can visit our product page and buy the herbal made supplements for achalasia.
What is GERD?
Gastroesophageal reflux disease (GERD) is a common condition in which stomach acid flows back into the esophagus, causing irritation and inflammation. Unlike achalasia, GERD is primarily caused by a malfunctioning lower esophageal sphincter that allows acid reflux but does not block food movement.
Causes of GERD
GERD has a multifactorial origin, including:
- Lower esophageal sphincter weakness: Often due to obesity, aging, or certain foods.
- Hiatal hernia: Stomach protruding through the diaphragm can worsen reflux.
- Delayed gastric emptying: Slow digestion increases acid exposure.
- Lifestyle factors: Smoking, alcohol, caffeine, and high-fat meals exacerbate symptoms.
- Medications: Certain drugs like NSAIDs, calcium channel blockers, or nitrates may relax the LES.
Symptoms of GERD
GERD symptoms often overlap with achalasia, which can complicate diagnosis:
- Heartburn: Burning sensation behind the breastbone.
- Regurgitation: Acidic or bitter taste in the mouth.
- Dysphagia: Usually mild and intermittent.
- Chronic cough or hoarseness: Due to acid irritation of the throat.
- Chest pain: Burning rather than spasm-related.
- Bloating and nausea: Sometimes present.
Unlike achalasia, GERD rarely causes significant weight loss unless severe complications like esophagitis or Barrett’s esophagus develop.
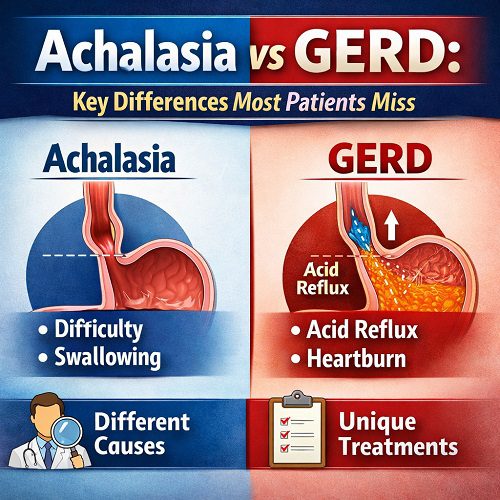
Comparing Achalasia vs GERD
Although achalasia vs GERD share some overlapping symptoms, the underlying pathophysiology, progression, and management are distinct. Understanding these differences helps avoid misdiagnosis.
| Feature | Achalasia | GERD |
| Cause | Nerve damage leading to LES non-relaxation | Weak LES, hiatal hernia, acid reflux |
| Onset | Gradual, progressive | Can be intermittent, often linked to meals |
| Swallowing difficulty | Severe for solids and liquids | Mild, often with solids |
| Regurgitation | Undigested food, non-acidic | Acidic, bitter taste |
| Chest pain | Esophageal spasm | Burning from acid |
| Weight changes | Often weight loss | Usually stable, weight gain possible |
| Heartburn | Rare or mild | Classic symptom |
| Nocturnal symptoms | Food aspiration | Acid reflux at night |
| Diagnostic test | Esophageal manometry, barium swallow | Endoscopy, pH monitoring |
Why Patients Often Confuse Achalasia with GERD
Several factors contribute to the confusion between achalasia vs GERD:
- Overlapping symptoms: Regurgitation, chest pain, and dysphagia appear in both.
- Mild early-stage achalasia: Initially, patients may experience only occasional swallowing difficulty, mimicking GERD.
- Self-treatment with antacids: Patients may temporarily relieve symptoms, masking achalasia.
- Delayed referral to specialists: Many patients assume heartburn is the cause, leading to prolonged treatment with proton pump inhibitors (PPIs) before correct diagnosis.
Diagnostic Strategies
Accurate diagnosis is critical for differentiating achalasia vs GERD.
Achalasia Diagnostics
- Esophageal manometry: Gold standard; measures pressure and relaxation of the LES.
- Barium swallow (esophagram): Shows a dilated esophagus and “bird-beak” narrowing at the LES.
- Endoscopy: Excludes structural obstruction or cancer.
GERD Diagnostics
- Upper endoscopy: Detects esophagitis, Barrett’s esophagus, or strictures.
- 24-hour pH monitoring: Measures acid exposure in the esophagus.
- Esophageal impedance testing: Detects reflux of non-acidic content.
- Response to therapy: Symptom improvement with PPIs supports GERD diagnosis.
Treatment Differences Between Achalasia and GERD
Management approaches for achalasia vs GERD differ due to their distinct pathophysiology.
Achalasia Treatment
- Endoscopic interventions:
- Pneumatic dilation: Stretching the LES with a balloon.
- Peroral endoscopic myotomy (POEM): Minimally invasive muscle incision to relax LES.
- Surgical options:
- Heller myotomy: Surgical cutting of LES muscles, often combined with fundoplication to prevent reflux.
- Medications (limited efficacy):
- Calcium channel blockers or nitrates to relax LES.
- Lifestyle modifications:
- Eating slowly, smaller meals, elevating head during sleep.
GERD Treatment
- Lifestyle changes:
- Avoid trigger foods, reduce alcohol, stop smoking, lose weight.
- Elevate the head of the bed.
- Medications:
- Antacids: Short-term relief.
- H2 receptor blockers: Moderate acid suppression.
- Proton pump inhibitors (PPIs): Long-term acid suppression.
- Surgery:
- Nissen fundoplication: Reinforces the LES in severe cases.
Complications if Misdiagnosed
Confusing achalasia vs GERD can lead to serious complications:
Achalasia Misdiagnosed as GERD
- Persistent dysphagia and regurgitation.
- Risk of aspiration pneumonia.
- Progressive esophageal dilation (megaesophagus).
- Rarely, esophageal cancer (squamous cell carcinoma).
GERD Misdiagnosed as Achalasia
- Unnecessary invasive procedures (e.g., myotomy).
- Persistent acid reflux causing esophagitis, Barrett’s esophagus, and stricture formation.
Lifestyle Considerations for Both Conditions
Although treatments differ, lifestyle management supports both conditions:
- Eat smaller, more frequent meals.
- Avoid late-night eating.
- Maintain a healthy weight.
- Avoid foods that trigger reflux (GERD) or are hard to swallow (achalasia).
- Opt for High-calorie soft foods for achalasia patients
- Quit smoking and limit alcohol.
Red Flags That Warrant Immediate Medical Attention
Patients should seek prompt evaluation if they experience:
- Sudden difficulty swallowing solids or liquids.
- Severe chest pain not relieved by antacids.
- Unintentional weight loss.
- Vomiting blood or black stools.
- Recurrent aspiration or choking.
These signs may indicate advanced achalasia, severe GERD, or another serious esophageal disorder.
Key Takeaways: Achalasia vs GERD
Understanding the differences between achalasia vs GERD can prevent misdiagnosis:
- Achalasia is primarily a motility disorder, GERD is an acid reflux disorder.
- Dysphagia in achalasia affects solids and liquids; in GERD, it is usually mild and intermittent.
- Regurgitation in achalasia is non-acidic and undigested, while GERD regurgitation is acidic.
- Weight loss is common in achalasia; heartburn is the hallmark of GERD.
- Diagnostic tests like esophageal manometry (achalasia) and pH monitoring (GERD) are essential.
Conclusion
While achalasia vs GERD share overlapping symptoms, their causes, progression, and management differ significantly. Misdiagnosis can lead to prolonged discomfort, ineffective therapy, and serious complications. Awareness of the subtle distinctions—especially regarding swallowing difficulties, type of regurgitation, and weight changes—can guide patients and physicians toward accurate diagnosis and appropriate treatment.
Patients with chronic esophageal symptoms should seek evaluation by a gastroenterologist for specialized testing. Early intervention not only improves quality of life but also prevents complications associated with untreated achalasia or uncontrolled GERD. Understanding these differences empowers patients to advocate for proper care, ensuring the best outcomes for their digestive health.