Achalasia is a rare but serious swallowing disorder that affects the esophagus—the muscular tube that carries food from the mouth to the stomach. Because its symptoms often resemble more common conditions like acid reflux or gastroesophageal reflux disease (GERD), obtaining an accurate achalasia diagnosis test is crucial for proper treatment.
Early and precise diagnosis can prevent complications such as weight loss, malnutrition, aspiration pneumonia, and severe esophageal dilation. We explains how achalasia is diagnosed, what tests are involved, and how doctors interpret the results. We will break down each diagnostic method—including endoscopy, barium swallow studies, and esophageal manometry—so you can understand what to expect.
Understanding Achalasia Before Diagnosis
Achalasia is a motility disorder of the esophagus. It occurs when:
- The lower esophageal sphincter (LES) fails to relax properly.
- The normal rhythmic contractions (peristalsis) of the esophageal muscles are lost.
As a result, food and liquids cannot move efficiently into the stomach. Instead, they accumulate in the esophagus. Achalasia occurs in different stages which we can say Mild vs Severe Achalasia.
Common Symptoms That Lead to Testing
Doctors usually begin investigating achalasia when patients report:
- Dysphagia caused in Achalasia, especially for both solids and liquids
- Regurgitation of undigested food
- Chest pain or discomfort
- Weight loss
- Persistent cough or choking at night
- Heartburn that does not respond to standard acid reflux medications
Because these achalasia symptoms overlap with other gastrointestinal disorders, physicians rely on specific achalasia diagnosis tests to confirm the condition.
Visit our Product Page: Achalasia Natural Treatment
Why Accurate Diagnosis Is So Important
Achalasia requires specialized treatment such as pneumatic dilation, surgical myotomy, or peroral endoscopic myotomy (POEM). These treatments differ significantly from therapies used for acid reflux.
Misdiagnosis can lead to:
- Ineffective treatment
- Progressive esophageal enlargement
- Increased risk of esophageal cancer (rare but possible in long-standing cases)
That’s why a structured diagnostic approach is essential.
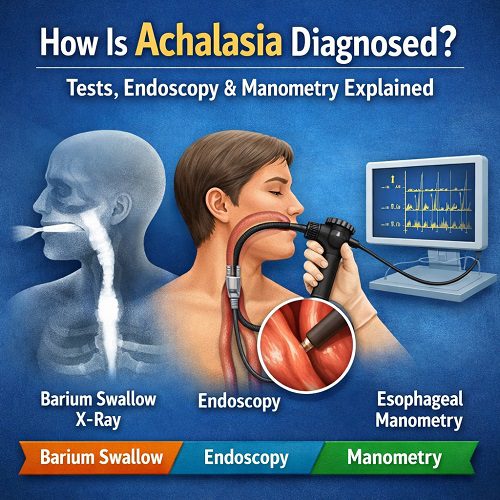
The Three Main Achalasia Diagnosis Tests
Most gastroenterologists rely on three core diagnostic tools:
- Barium swallow (esophagram)
- Upper endoscopy (EGD)
- Esophageal manometry (gold standard test)
Often, these tests are performed in combination to confirm the diagnosis and rule out other conditions.
Let’s examine each in detail.
1. Barium Swallow (Esophagram)
What Is It?
A barium swallow is an imaging test that uses X-rays to visualize the esophagus. The patient drinks a chalky liquid containing barium sulfate, which coats the lining of the esophagus and makes it visible on X-ray images.
Why It’s Used in Achalasia Diagnosis
This test helps doctors see:
- Delayed emptying of the esophagus
- Narrowing at the lower esophageal sphincter
- Esophageal dilation (widening)
- Absence of normal peristalsis
Classic Findings in Achalasia
The most characteristic sign is the “bird’s beak” appearance:
- The lower esophagus narrows sharply at the LES.
- The upper portion becomes widened due to retained food and fluid.
What to Expect During the Test
- You will stand or lie on an exam table.
- You will swallow barium liquid.
- Multiple X-ray images will be taken.
- The test usually takes 20–30 minutes.
Pros and Limitations
Advantages:
- Non-invasive
- Provides structural information
- Shows severity of dilation
Limitations:
- Cannot directly measure muscle pressure
- May not detect early-stage achalasia
- Cannot distinguish subtypes of achalasia
While helpful, a barium swallow alone cannot definitively confirm achalasia. It often leads to the next step: endoscopy or manometry.
2. Upper Endoscopy (EGD)
What Is an Endoscopy?
Upper endoscopy—also called esophagogastroduodenoscopy (EGD)—involves inserting a flexible tube with a camera through the mouth into the esophagus and stomach.
Why It’s Important in Achalasia Diagnosis
Endoscopy serves two major purposes:
- Rule out mechanical obstruction, such as tumors or strictures.
- Evaluate the internal appearance of the esophagus.
In some cases, a cancer near the lower esophagus can mimic achalasia. This condition is known as pseudoachalasia, and it must be ruled out.
What Doctors Look For
During endoscopy, physicians may observe:
- Retained food or saliva in the esophagus
- Dilated esophagus
- Tight lower esophageal sphincter
- Inflammation or irritation
- Difficulty passing the scope into the stomach
What to Expect During the Procedure
- Performed under sedation
- Takes about 15–30 minutes
- Minimal discomfort due to sedation
- You will need someone to drive you home
Why Endoscopy Alone Isn’t Enough
While endoscopy can strongly suggest achalasia, it cannot measure esophageal muscle contractions. That is why manometry remains the definitive achalasia diagnosis test.
3. Esophageal Manometry (The Gold Standard)
What Is Esophageal Manometry?
Esophageal manometry measures the pressure and coordination of esophageal muscles during swallowing.
It is considered the most important achalasia diagnosis test because it directly evaluates esophageal function.
How It Works
A thin, flexible catheter is passed through the nose into the esophagus. The tube contains pressure sensors that measure:
- Muscle contractions
- Lower esophageal sphincter pressure
- LES relaxation during swallowing
You will be asked to swallow small amounts of water while the system records pressure changes.
What Manometry Shows in Achalasia
Diagnostic criteria include:
- Incomplete relaxation of the LES
- Absence of normal peristalsis
- Elevated resting LES pressure (in many cases)
High-Resolution Manometry (HRM)
Modern testing uses high-resolution manometry, which provides detailed pressure maps. HRM allows doctors to classify achalasia into three subtypes:
Type I (Classic Achalasia)
- Minimal esophageal pressurization
- No peristalsis
Type II (Achalasia with Compression)
- Simultaneous pressurization of the esophagus
- Best treatment response
Type III (Spastic Achalasia)
- Premature or spastic contractions
- Often associated with chest pain
Subtyping is critical because it influences treatment decisions.
What to Expect During the Test
- Usually performed without sedation
- Takes about 30–45 minutes
- Mild discomfort in the nose or throat
- Temporary gagging sensation possible
Though slightly uncomfortable, it is safe and highly informative.
Additional Tests That May Be Used
While the three main tests form the core of achalasia diagnosis, doctors sometimes use additional studies.
Timed Barium Esophagram
A variation of the standard barium swallow, this test measures how much barium remains in the esophagus at specific time intervals (1, 2, and 5 minutes). It helps assess severity and treatment response.
CT Scan or Endoscopic Ultrasound
If pseudoachalasia is suspected, imaging may be ordered to look for:
- Tumors
- External compression
- Enlarged lymph nodes
These tests are not routine for all patients.
The Step-by-Step Diagnostic Process
Here’s how the diagnostic pathway typically unfolds:
Step 1: Clinical Evaluation
- Review of symptoms
- Medical history
- Physical examination
Step 2: Initial Imaging
- Barium swallow often ordered first
Step 3: Endoscopy
- Rule out cancer or structural obstruction
Step 4: Manometry
- Confirm diagnosis
- Classify subtype
Only after these steps can doctors confidently confirm achalasia.
Differentiating Achalasia from Other Conditions
An accurate achalasia diagnosis test must distinguish it from:
GERD (Acid Reflux)
- GERD shows normal peristalsis
- LES pressure often low, not high
Esophageal Stricture
- Mechanical narrowing visible on endoscopy
Esophageal Cancer
- Irregular mass or lesion
- Weight loss more rapid
Diffuse Esophageal Spasm
- Intermittent normal peristalsis
- Different manometry pattern
Proper testing ensures these conditions are not confused with achalasia.
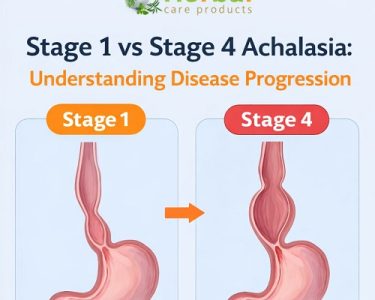
Early vs. Advanced Achalasia: Diagnostic Differences
Early Stage
- Mild dilation
- Subtle manometry abnormalities
- Symptoms may be intermittent
Advanced Stage
- Marked esophageal enlargement
- Sigmoid-shaped esophagus
- Severe food retention
- Clear manometric findings
Early diagnosis can significantly improve long-term outcomes.
Risks and Safety of Diagnostic Tests
Most achalasia diagnosis tests are safe.
Barium Swallow
- Minimal radiation exposure
- Rare constipation from barium
Endoscopy
- Small risk of bleeding or perforation
- Sedation-related risks (rare)
Manometry
- Mild discomfort
- Very low complication rate
Overall, benefits far outweigh risks.
When Should You See a Doctor?
Seek medical evaluation if you experience:
- Persistent swallowing difficulty
- Food getting stuck
- Unexplained weight loss
- Regurgitation of undigested food
- Chronic cough without clear cause
Early testing leads to faster relief.
How Long Does Diagnosis Take?
From first appointment to confirmed diagnosis, it may take:
- A few weeks in straightforward cases
- Longer if symptoms are subtle or misattributed to reflux
Advocating for proper testing is important if symptoms persist.
The Importance of Specialized Care
Because achalasia is rare, diagnosis is often best managed by:
- Gastroenterologists
- Esophageal motility specialists
- Centers with high-resolution manometry capability
Specialized centers improve diagnostic accuracy and treatment success.
Frequently Asked Questions
Is manometry always required?
Yes, in most cases. It is the definitive achalasia diagnosis test and confirms functional abnormalities.
Can achalasia be diagnosed with blood tests?
No. Blood tests do not detect achalasia.
Does endoscopy hurt?
No. It is performed under sedation, so patients typically feel little to no discomfort.
Can achalasia be missed?
Yes. Early-stage achalasia may be misdiagnosed as GERD unless proper testing is performed.
Final Thoughts
Achalasia is a complex but treatable esophageal disorder. Because its symptoms mimic more common digestive problems, proper testing is essential.
The most reliable approach to diagnosis involves:
- Barium swallow imaging
- Upper endoscopy
- High-resolution esophageal manometry (gold standard)
If you or someone you know experiences persistent difficulty swallowing, don’t ignore it. A thorough achalasia diagnosis test can lead to effective treatment and significantly improve quality of life.
Early detection prevents complications, guides appropriate therapy, and ensures long-term esophageal health.